
Breast
Reconstruction
IN DUBAI
Restoring breast form through personalized reconstructive techniques.
RESTORATIVE BREAST RECONSTRUCTION SURGERY
Breast reconstruction restores breast form after mastectomy or previous breast procedures using tailored reconstructive techniques.
DR. IRAJ
overview
Breast reconstruction restores the shape of the breast following mastectomy or other breast cancer surgery.
For many women, reconstruction represents an important part of recovery after breast cancer. The goal of reconstruction is to recreate a breast that looks natural, feels balanced with the rest of the body and allows patients to move forward with confidence.
Modern breast reconstruction can be performed using:
• implant-based reconstruction
• autologous tissue reconstruction using the patient’s own tissue
The most appropriate approach depends on the patient’s anatomy, cancer treatment and personal preferences.
The Reconstruction Journey
Breast reconstruction is often best understood as a journey rather than a single operation.
While some women complete their reconstruction in one stage, many reconstructions are performed over several steps to achieve the best possible result.
This process may involve:
• the initial reconstruction at the time of mastectomy or at a later stage
• refinement procedures to improve shape and contour
• fat grafting to optimise soft tissue quality
• nipple reconstruction and areola restoration
• balancing procedures on the opposite breast when required
Each stage of reconstruction is carefully planned so that the final result appears natural and balanced.
The aim is not simply to recreate a breast, but to restore a sense of normality and confidence following breast cancer treatment.
Each stage of reconstruction is planned carefully to achieve a result that restores both form and balance while respecting the patient’s cancer treatment journey.
Specialist Breast Reconstruction Surgery
Dr Iraj Ahmadi is a plastic surgeon with specialist training in breast reconstruction, including microsurgical breast reconstruction techniques.
He is one of a small number of surgeons in the UAE performing advanced procedures such as the Deep Inferior Epigastric Perforator Flap, which uses a patient’s own abdominal tissue to recreate the breast.
These procedures require specialized microsurgical techniques to reconnect blood vessels and restore living tissue to the reconstructed breast.
Complex breast reconstruction cases are managed through the breast multidisciplinary team (MDT) at Mediclinic, ensuring that treatment planning aligns with international standards of breast cancer care.
Timing of Breast Reconstruction
Breast reconstruction can be performed at different stages of breast cancer treatment.
Immediate Reconstruction
Reconstruction may be performed at the same time as mastectomy. This approach can allow the breast to be reconstructed during the same operation as cancer removal.
Delayed Reconstruction
In some situations, reconstruction may be performed at a later stage, particularly if additional treatments such as radiotherapy are required.
The timing of reconstruction is carefully planned in coordination with the breast cancer treatment team.
Types of Breast Reconstruction
Modern breast reconstruction can be performed using either breast implants or the patient’s own tissue.
The most appropriate approach depends on the individual patient, the type of cancer treatment required and the patient’s anatomy and preferences.
Both approaches can achieve excellent outcomes when carefully planned.
Implant-Based Reconstruction
Implant reconstruction recreates the breast shape using a breast implant.
In selected patients this can be performed as a direct-to-implant reconstruction (DTI) at the time of mastectomy. In this situation the implant is placed during the same operation as the cancer surgery.
Supportive materials such as surgical mesh, including products like Galaflex, may be used to provide additional support and help shape the reconstructed breast.
In other situations, reconstruction may be performed in two stages. The first stage involves placement of a tissue expander, which gradually prepares the tissues for the final implant. Once cancer treatments such as chemotherapy or radiotherapy have been completed, the expander can be exchanged for a permanent implant.
Both approaches can provide very good aesthetic outcomes when carefully selected for the individual patient.
Autologous (Microsurgical) Breast Reconstruction
Autologous reconstruction uses the patient’s own tissue to recreate the breast.
This is commonly performed using microsurgical techniques, where tissue from another part of the body is transferred to the chest and the blood vessels are reconnected under a microscope.
One of the most advanced techniques is the Deep Inferior Epigastric Perforator (DIEP) flap, which uses tissue from the lower abdomen to reconstruct the breast while preserving the abdominal muscles.
Because the reconstruction uses living tissue, it can:
• feel soft and natural
• adapt to changes in body weight over time
• provide a long-lasting reconstruction
In some situations, other flap options may be considered, including:
• gracilis flaps from the inner thigh
• latissimus dorsi flaps from the back
These options are less commonly used but can be appropriate in certain patients depending on anatomy and prior treatments.
surgeon insight
Autologous flap reconstruction is widely considered the gold standard for breast reconstruction internationally. Because the reconstruction uses the patient’s own tissue, it behaves similarly to natural breast tissue and can provide a lifelong reconstruction.
AT A GLANCE
Overnight Stay
O DAYS
Final Result
6 MONTHS
Anaesthetic
Duration
1-2 HRS
GENERAL
Adjunct Procedures in Breast Reconstruction
Breast reconstruction is often completed in stages to refine the final result and restore balance between the breasts.
Additional procedures may include:
• fat grafting, which improves contour and soft tissue quality
• nipple reconstruction, to recreate the nipple and areola
• symmetrising procedures on the opposite breast, such as reduction or lift surgery to achieve balance
These procedures allow the reconstruction to be refined so that the final outcome appears natural and proportionate.
Surgical Planning
Planning breast reconstruction requires careful consideration of several factors including:
• the type of breast cancer surgery required
• the need for radiotherapy or other treatments
• the patient’s anatomy
• personal preferences regarding reconstruction
The treatment plan is developed in collaboration with the breast cancer multidisciplinary team (MDT) to ensure that reconstruction aligns with the overall cancer treatment plan.
BEFORE AND AFTER
See before and after photos of a successful Breast Reconstruction Surgery.
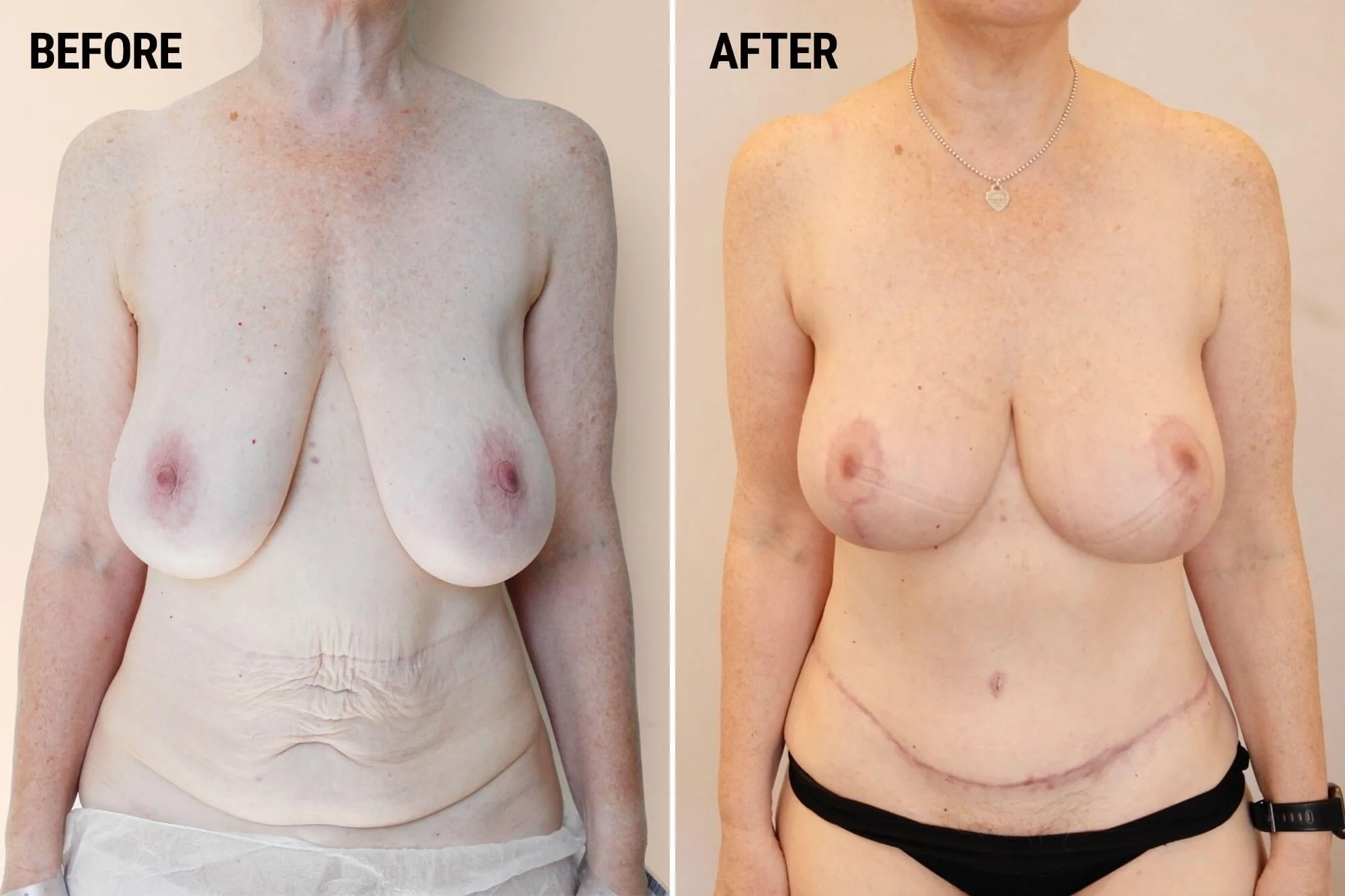
Comparison of a woman’s torso before and after breast reconstruction surgery. The left shows a woman with natural breasts, loose skin, and signs of aging. The right shows the same woman with reconstructed breasts, scars visible beneath the breasts, and wearing black underwear.

Side-by-side comparison of a woman's torso before and after breast reconstruction surgery. The left image shows her with natural breasts, loose skin, and visible signs of aging. The right image shows her with reconstructed breasts, some scarring, and wearing black underwear and a necklace.
Recovery
Recovery following breast reconstruction varies depending on the technique used.
Implant-based reconstruction generally involves shorter operative time and recovery.
Microsurgical reconstruction procedures such as DIEP flap reconstruction involve longer operations and a more involved recovery period because living tissue is transferred and reconnected.
Typical recovery milestones may include:
• several days of hospital monitoring following microsurgical reconstruction
• gradual return to light activities over the following weeks
• progressive improvement in comfort and mobility as healing progresses
Follow-up appointments allow the reconstruction to be monitored as healing continues.
Results
Breast reconstruction restores the contour of the breast following cancer surgery.
When carefully planned the aim is to achieve a breast that looks natural and balanced with the rest of the body.
Autologous reconstruction using the patient’s own tissue often provides the most natural long-term result, as the reconstructed breast behaves similarly to normal breast tissue.
FAQs
-
Breast reconstruction is surgery that restores the shape of the breast after mastectomy or other breast cancer treatment.
-
A DIEP flap is a type of breast reconstruction that uses tissue from the lower abdomen to recreate the breast.
-
Autologous reconstruction using a patient’s own tissue is often considered the gold standard because the reconstruction behaves like natural breast tissue.
-
Yes. Many patients choose immediate reconstruction performed during the same operation as cancer removal.
-
Recovery depends on the technique used. Microsurgical reconstruction procedures require longer recovery than implant-based reconstruction.
-
Reconstruction using a patient’s own tissue often provides the most natural feel.
-
Yes. When reconstruction uses the patient’s own tissue, the breast can change with body weight over time.
-
No. Many reconstructions can be performed using the patient’s own tissue.
-
Yes. Reconstruction is commonly performed as part of breast cancer treatment planning.
-
Patients undergoing mastectomy or breast cancer surgery may be candidates for reconstruction depending on their treatment plan and personal goals.
GET TO KNOW
DR. IRAJ.
Dr Iraj Ahmadi is a specialist plastic and reconstructive surgeon whose work bridges aesthetic refinement and complex reconstructive surgery.
Alongside this work, his practice spans aesthetic surgery of the face and body as well as reconstructive surgery for cancer, trauma and complex tissue loss.
Related procedures
-

Breast Lift
-

Breast Reduction
-

Breast Implant Removal
-

Breast Augmentation